Blog
Adenoids & Adenoiditis: Comprehensive Guide to Symptoms, Treatment & Recovery
Adenoids & Adenoiditis: Your Comprehensive Guide to Symptoms, Treatment & Recovery
Is your child’s persistent snoring more than just a nuisance? Are frequent ear infections or chronic mouth breathing becoming a concern? You might be encountering issues with their adenoids. While often misspelled as “adenoidid,” the correct terms, “adenoids” and “adenoiditis,” refer to a common childhood condition that can significantly impact a child’s health and development. This comprehensive guide delves into everything you need to know about these crucial immune tissues, from their function and common problems to the latest diagnostic methods and cutting-edge treatment options. We’ll explore how to identify the signs, understand the causes, and navigate the path to better health, ensuring your child breathes easier and sleeps sounder.
Understanding Adenoids: The Body’s Hidden Guardians
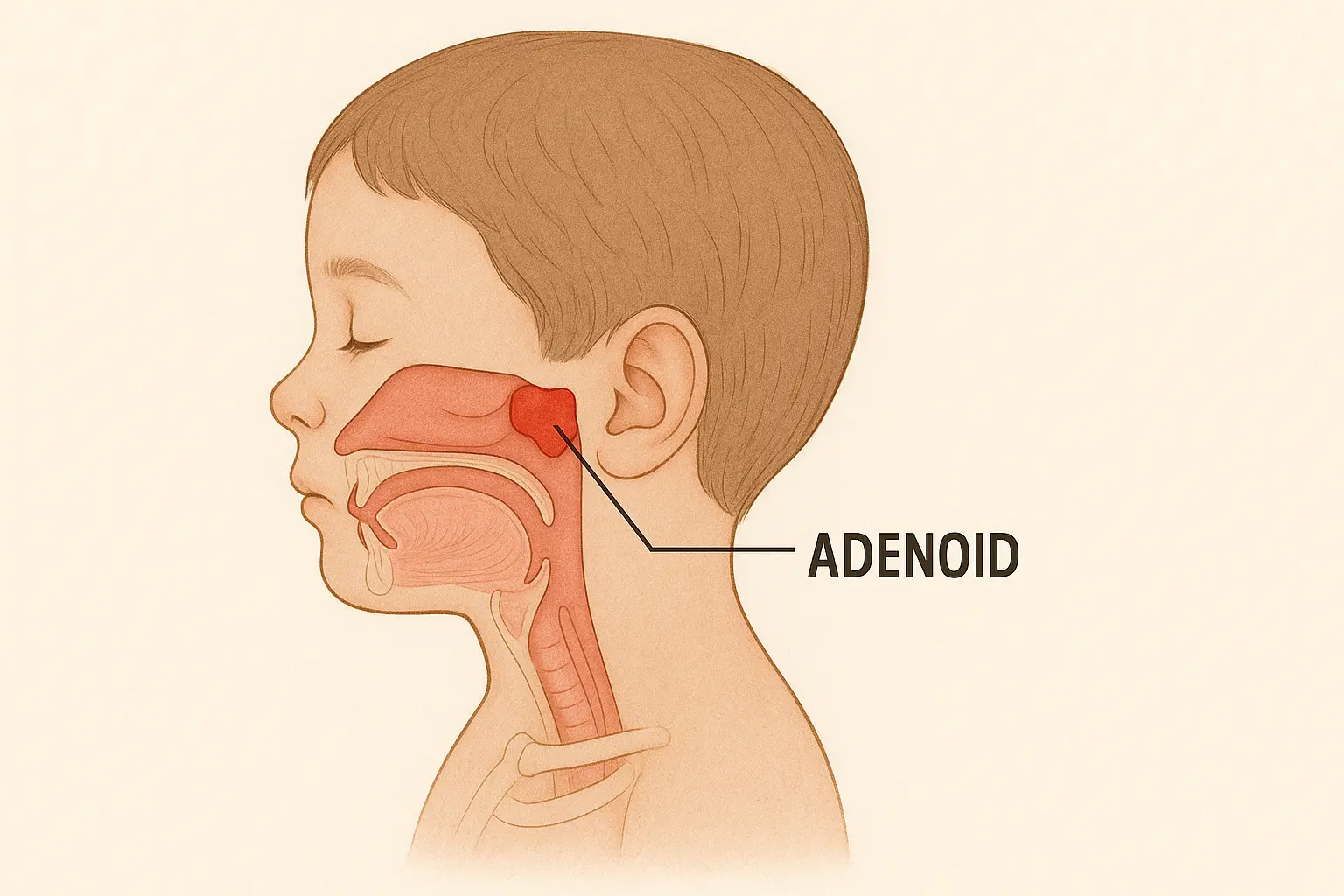
Nestled high in the throat, just behind the nasal passage, are the adenoids—a small, rectangular mass of lymphatic tissue. Along with the tonsils, they form a vital part of the body’s immune system, acting as a first line of defense against harmful germs that enter through the mouth and nose.
What Are Adenoids and What Do They Do?
Adenoids are present from the seventh month of gestation and play a crucial role in developing immunologic memory throughout childhood. They function by trapping pathogens like bacteria and viruses, and their immune cells produce antibodies to neutralize these threats before they can spread. This “priming” of the immune system is particularly important in infancy.
Normal Development and When They Shrink
Adenoids typically grow to their maximum size between ages 3 and 5, reaching peak size by age 7. After this period, they usually begin to shrink, often disappearing almost completely by the teenage years. By adulthood, the body develops other robust ways to fight infections, making the adenoids less critical.
Enlarged Adenoids (Adenoid Hypertrophy) & Adenoiditis
While adenoids are essential for early childhood immunity, they can sometimes become enlarged or inflamed, leading to a range of health issues.
What Are Enlarged Adenoids (Adenoid Hypertrophy)?
Adenoid hypertrophy (AH) refers to the abnormal enlargement of the adenoid tissue. This is a common condition in children, with a meta-analysis reporting an overall prevalence of 49.70%. In randomized, representative populations, the prevalence is around 34.46%. AH is most commonly seen in children aged 0-5 years (54.7% of cases) and 3–6 years.
What Is Adenoiditis?
Adenoiditis is the inflammation of the adenoid tissue, most commonly resulting from infection, allergies, or irritation from stomach acid (laryngopharyngeal reflux). It rarely occurs independently and is typically part of a broader regional disease process, such as adenotonsillitis or rhinosinusitis. Chronic adenoiditis, lasting at least 90 days, is often caused by polymicrobial infections and biofilm formation.
Causes of Enlarged Adenoids and Adenoiditis
Enlargement of the adenoids is often a natural immune response to fight off infections. However, in some children, the adenoids remain swollen even after the infection clears. Common causes include:
Infections
Bacterial (e.g., Haemophilus influenza) or viral (e.g., adenovirus) infections. Chronic cases can result from biofilm development.
Allergies
Conditions like allergic rhinitis and exposure to allergens such as house dust can contribute to persistent hypertrophy.
Acid Reflux
Irritation from stomach acid, as seen in laryngopharyngeal reflux, can cause inflammation.
Congenital Factors
Some children are born with naturally larger adenoids, predisposing them to issues.
Environmental Irritants
Exposure to cigarette smoke (passive smoking) and emerging links to outdoor air pollution (PM2.5).
Symptoms of Enlarged Adenoids: Recognizing the Signs
Enlarged adenoids primarily affect the upper respiratory system, with symptoms often more noticeable at night. Since adenoids cannot be seen by looking into the mouth, recognizing these signs is crucial.
Common Symptoms in Children
Difficulty Breathing Through Nose
A hallmark symptom, often leading to chronic mouth breathing.
Mouth Breathing
Can lead to dry mouth, cracked lips, and bad breath.
Snoring & Noisy Breathing
Often described as “Darth Vader” breathing. Snoring is a significant warning sign.
Frequent Ear Infections
Obstruction of the Eustachian tube can lead to fluid buildup (glue ear) and hearing loss.
Nasal Speech (Hyponasality)
The voice may sound pinched or as if talking through a blocked nose.
Chronic Sinus Infections & Runny Nose
Persistent nasal discharge or congestion.
Less Common but Significant Symptoms
- “Adenoid Facies” (Long-Face Syndrome): Chronic mouth breathing due to enlarged adenoids can lead to distinct facial changes, including narrowed maxillary and dental arches, upper lip incompetence, and a posterior-rotated mandible. This visually distinct symptom is a key indicator of long-standing issues.
- Bedwetting (Enuresis): Can be a complication of disrupted sleep due to adenoid hypertrophy.
- Cognitive Delays & Behavioral Issues: Untreated adenoid hypertrophy can lead to oxygen deprivation during sleep, affecting brain and nervous system function, resulting in poor academic performance, hyperactivity, low intelligence quotient, and learning and behavioral problems.
Diagnosing Adenoid Issues
If you suspect your child has enlarged adenoids, a medical professional can accurately diagnose the condition.
Initial Assessment
Diagnosis typically begins with a thorough medical history review, including your child’s symptoms, and a physical examination of their ears, nose, and throat. Since adenoids are high up behind the nose, they cannot be seen by simply looking into the mouth.
Diagnostic Tools
- Special Mirror or Endoscope: A small mirror or a long, flexible tube with a light and camera (endoscope) can be inserted into the nasal passage to directly visualize the adenoids and check for redness, inflammation, or enlargement.
- Imaging Tests: X-rays (especially lateral neck radiography to assess the adenoid-nasopharyngeal ratio, A/N ratio), CT scans, or MRI may be used to get a better view of the nasal passages, sinuses, and adenoids. CT or MRI are considered when there’s a high suspicion of other conditions like angiofibroma or cancer.
- Sleep Study (Polysomnogram): If enlarged adenoids are suspected of causing obstructive sleep apnea or significant snoring, a sleep study may be recommended to define the severity of sleep disturbance.
- Bacteria Culture Test: A throat culture may be taken to determine if a bacterial infection is causing the enlargement.
Treatment Options for Enlarged Adenoids and Adenoiditis
Treatment for enlarged adenoids depends on the underlying cause, severity of symptoms, and frequency of infections.
Watchful Waiting
If symptoms are mild or resolve naturally, a “watchful waiting” approach may be recommended, as adenoids often shrink as a child grows older.
Medical Management
- Nasal Steroid Sprays: Medications like intranasal mometasone furoate or fluticasone spray can help reduce swelling in the adenoids. A 2024 prospective study showed a maximal medical treatment regimen (including intranasal mometasone furoate, decongestion drops, oral desloratadine, nasal saline irrigation, and bacteriotherapy) resulted in clinical improvement in 72% of preschool children with adenoid hypertrophy symptoms.
- Antibiotics: Prescribed if a bacterial infection (e.g., strep throat) is responsible for the enlargement or inflammation. A clinical trial found azithromycin suspension to be more effective than fluticasone spray for short-term improvements in apnea and hyponasal speech.
- Antihistamines: For allergies contributing to enlargement.
- Reflux Treatment: To manage irritation from stomach acid.
When Is Surgery Recommended?
If non-surgical methods don’t resolve the issue, or if symptoms are severe and persistent, an adenoidectomy (surgical removal of the adenoids) may be recommended. Common reasons for surgery include:
- Repeated or Chronic Infections: Especially if they lead to frequent ear or sinus infections, or if infections don’t respond to antibiotics.
- Significant Airway Blockage: Causing trouble breathing through the nose, loud snoring, or obstructive sleep apnea.
- Trouble Swallowing or Nasal Speech: If these issues significantly impact daily life.
- Tumor in the Throat or Nasal Passage: Though rare, this can be a reason for removal.
Adenoidectomy: Surgical Removal
Adenoidectomy is one of the most common surgical procedures performed on children.
What Is an Adenoidectomy?
An adenoidectomy is the surgical removal of the adenoids. It’s typically an outpatient procedure performed under general anesthesia, meaning your child will be asleep and won’t feel any pain. The surgeon removes the adenoids through the mouth, with no external cuts or scars. The procedure usually takes about 20-30 minutes.
Types of Adenoidectomy
Surgeons may use various techniques, including traditional instruments, cautery (using heat or electrical energy to remove tissue and seal blood vessels), or radiofrequency energy. While some studies compare “hot” (cautery) and “cold” (traditional cutting) techniques, finding mixed results regarding operation times, blood loss, and complication rates, overall complication rates are generally low.
Adenoidectomy vs. Tonsillectomy
Adenoids and tonsils are often removed at the same time in a procedure called an adenotonsillectomy (T&A). This is common because both tissues can contribute to airway obstruction or recurrent infections. However, an adenoidectomy can also be performed alone, especially if the primary issues are nasal obstruction or recurrent ear infections.
Recovery After Adenoidectomy: A Parent’s Guide
Recovery from an adenoidectomy is generally quick, with most children feeling better within a few days to a week. Most children are hospitalized for only 1-2 days post-surgery (83.16% in a 2024/2025 study).
Immediate Post-Op & Day-by-Day Recovery Timeline
Pain Management
Administer pain medicine (acetaminophen or ibuprofen) as directed. Avoid aspirin. Pain typically lasts 3-4 days.
Fluid Intake
Encourage plenty of fluids like popsicles, water, and soup to prevent dehydration. Drinking is crucial.
Diet
Start with soft foods like pudding, soup, and mashed potatoes. Return to a usual diet within a few days.
Rest & Activity
Keep your child home from school for about a week. Avoid heavy or rough play.
Comfort Measures
A cool-mist humidifier can help soothe a stuffy nose. Clean it daily.
When to Call the Doctor
Call your doctor now or seek immediate medical care if your child:
- Has a new or higher fever.
- Has any trouble breathing or difficulty breathing that gets worse.
- Has neck pain or stiffness that doesn’t go away with pain medicine.
- Refuses to drink or shows signs of dehydration.
- Has blood dripping from the nose or coating the tongue for more than 10 minutes.
- Vomits blood or something that looks like coffee grounds.
Risks and Potential Complications of Adenoidectomy
Adenoidectomy is a common and generally safe procedure. However, like any surgery, it carries some potential risks and complications:
- Bleeding: A small number of children (8.16% in a 2024/2025 study) may experience bleeding after a T&A, which can happen up to two weeks post-surgery and may require a second operation. Postoperative bleeding rates have significantly declined to as low as 0.07% with modern techniques.
- Temporary Voice Change: The voice may sound nasal for a few weeks.
- Infection: Infection at the surgical site is possible (6.63% in a 2024/2025 study), but antibiotics can help.
- Damage to Teeth: Rare, but the surgeon might chip or knock a tooth, especially if it’s loose or capped.
- Velopharyngeal Insufficiency (VPI): A rare but serious complication (1 in 1,500 to 1 in 10,000 cases) where the soft palate cannot properly seal against the back of the throat, leading to hypernasal speech. This is more likely if the child has a short soft palate or a submucous cleft palate, which should be checked before surgery.
- Atlantoaxial Subluxation (Grisel Syndrome): An extremely rare but serious complication involving the neck vertebrae.
- Persistent Symptoms or Adenoid Regrowth: While uncommon, adenoids can sometimes grow back after surgery, or symptoms may persist.
Long-Term Outcomes and Benefits
Despite the potential for minor complications, the benefits of adenoidectomy, particularly for children with significant symptoms, are clear and often lead to lifelong health improvements.
- Significant Improvements in Breathing & Sleep: Adenoidectomy effectively reduces snoring and resolves obstructive sleep apnea in a high percentage of cases (85% improvement in sleep apnea symptoms). This leads to more restful sleep and improved overall health.
- Reduction in Infections: Children often experience fewer ear, nose, and throat infections, including chronic sinus infections. One study showed children who had an adenotonsillectomy had one-third fewer healthcare provider visits and needed half the prescriptions in the year after surgery.
- Positive Impact on Development: Beyond just breathing, adenotonsillectomy has been shown to significantly improve memory and learning in children with obstructive sleep apnea syndrome (OSAS), indicating positive neurocognitive benefits. It also leads to substantial improvements in behavioral issues and overall quality of life compared to watchful waiting. This is a crucial long-term benefit that extends beyond physical health.
- No Negative Effect on Overall Immunity: Despite being part of the immune system, removing adenoids does not negatively affect the body’s ability to fight infections, as the immune system has many other ways to fight germs.
Adenoids in Adulthood & Emerging Research
Adenoids in Adulthood: A Less Common Concern
While adenoids typically shrink by the teenage years, persistence of adenoid tissue into adulthood is an uncommon clinical finding. However, if adults present with symptoms of nasal obstruction, adenoid disease requires investigation. Enlarged adenoids in adults can be due to chronic infection, allergies, pollution, or smoking. Dedicated, comprehensive sections on adult adenoid issues are less common in general health content, making this an important area for a complete guide.
Emerging Research & Future Directions
- Environmental Factors: Studies are exploring the impact of chronic exposure to outdoor air pollution (e.g., PM2.5) on immune markers in youth, suggesting a potential link to adenoid inflammation. This highlights the importance of environmental health in understanding conditions like adenoid hypertrophy.
- Microbiome Connection: Preliminary studies are examining differences in the salivary microbiome in pediatric tonsillar hypertrophy patients, suggesting that the site of upper airway obstruction may influence the oral microbiome. This opens new avenues for understanding and potentially treating upper airway issues.
- Standardized Diagnosis & Treatment: Ongoing clinical trials, such as one estimated to start in May 2025, are investigating the precise correlation between adenoid hypertrophy size and middle ear effusion. The aim is to provide evidence for a more standardized approach to the diagnosis and treatment of Otitis Media with Effusion (OME). This research could lead to more consistent and effective management strategies.
Frequently Asked Questions (FAQs)
A: Recent research, including studies on adenotonsillectomy, indicates that early surgical intervention can lead to improvements in neurocognitive functioning, including memory and learning, in children with obstructive sleep apnea syndrome. While concerns about general anesthesia and IQ have been raised, current evidence suggests positive neurocognitive benefits from addressing OSAS.
A: No, removing adenoids does not negatively affect the body’s overall ability to fight infections. The immune system has many other ways to fight germs, and the adenoids become less important as a child gets older.
A: While rare, adenoids can sometimes grow back after surgery. However, most children who undergo adenoid removal will recover without any long-term health issues.
A: “Adenoid facies” describes specific facial changes seen in children with chronic adenoid hypertrophy. It’s believed to result from persistent mouth breathing due to nasal obstruction, leading to issues with dental and maxillofacial development, such as narrowed dental arches and a posterior-rotated mandible.
A: Adenoidectomy is a common and straightforward procedure, and complications are rare. A 2024/2025 study reported an overall postoperative complication rate of 26.53%, including minor issues like poor eating/drinking (11.73%) and infection (6.63%), with bleeding at 8.16%. Serious complications like long-term velopharyngeal insufficiency are very rare (1 in 1,500 to 1 in 10,000 cases).
A: Yes, for many children, medical management can be effective. This includes nasal steroid sprays, antibiotics for bacterial infections, antihistamines for allergies, and treatments for acid reflux. A 2024 study showed a maximal medical treatment regimen resulted in clinical improvement in 72% of preschool children.
Resource Appendix: Latest Data & Statistics Summary
| Statistic/Data Point | Value/Finding | Publication/Update Date | Significance/Context |
|---|---|---|---|
| Overall AH Prevalence | 49.70% (CI: 39.92-59.50) | 2017 (Meta-analysis) | General prevalence across studies. |
| AH Prevalence (Randomized Samples) | 34.46% | 2017 (Meta-analysis) | More representative prevalence. |
| AH Age Distribution (0-5 years) | 54.7% of cases | 2023 | Highlights prevalence in early childhood. |
| AH Age Distribution (6-10 years) | 25.0% of cases | 2023 | Continued prevalence in school-age children. |
| Adenoidectomy Unplanned Admission Rate | 2.3% | 2010-2023 study | Indicates low rate of unexpected hospital stays. |
| Postoperative Bleeding Rate (Modern Techniques) | As low as 0.07% | Recent decline | Demonstrates safety improvements in surgery. |
| Overall Postoperative Complication Rate | 26.53% (including bleeding, poor eating, infection) | 2024/2025 study | Provides a realistic overview of minor complications. |
| Post-Adenoidectomy Hospitalization (1-2 days) | 83.16% of children | 2024/2025 study | Most children go home quickly after surgery. |
| Medical Treatment Clinical Improvement Rate | 72% of preschool children | 2024 study | Shows high efficacy of non-surgical options. |
| Adenotonsillectomy Impact on Memory/Learning | Enhanced memory and learning in OSAS children | Recent research | Crucial long-term neurocognitive benefit. |
| Adenotonsillectomy Impact on Behavior/QoL | Significantly improves behavioral issues and quality of life | Recent research | Holistic benefits beyond breathing. |
| Adenoid Hypertrophy & OME Correlation Study | Ongoing clinical trial | Est. Start: May 2025 | Emerging research for standardized diagnosis/treatment. |
| Air Pollution & Immune Markers in Youth | Chronic exposure linked to higher anti-inflammatory markers | Recent research | Emerging environmental factor for adenoid health. |